PRINCIPLES USED FOR ALLOCATING/RATIONING SCARCE MEDICAL INTERVENTION”
Dr. Ezekiel Emanuel, “Dr. Death”
Coauthored by Dr. Ezekiel Emanuel
Allocation of medical interventions is a persistent ethical challenge. We evaluate eight simple allocation principles that can be classified into four categories: treating people equally, favouring the worst-off, maximising total benefits, and promoting and rewarding social usefulness. No single principle is sufficient to incorporate all morally relevant considerations and therefore individual principles must be combined into multiprinciple allocation systems. We evaluate three systems: the United Network for Organ Sharing points systems, quality-adjusted life-years, and disability-adjusted life-years. We recommend an alternative system—the complete lives system—which prioritises younger people who have not yet lived a complete life, and also incorporates prognosis, save the most lives, lottery, and instrumental value principles.
snip
Youngest first:
Although not always recognised as such, youngest-first allocation directs resources to those who have had less of something supremely valuable—life-years. Dialysis machines and scarce organs have been allocated to younger recipients first, and proposals for allocation in pandemic influenza prioritise infants and children. Daniel Callahan has suggested strict age cut-offs for scarce life-saving interventions, whereas Alan Williams has suggested a system that allocates interventions based on individuals’ distance from a normal life-span if left unaided.
snip
Prognosis or life-years:
Rather than saving the most lives, prognosis allocation aims to save the most life-years.
This strategy has been used in disaster triage and penicillin allocation, and motivates the exclusion of people with poor prognoses from organ transplantation waiting lists. Maximising life-years has intuitive appeal. Living more years is valuable, so saving more years also seems valuable.
http://tinyurl.com/noxjfc
"Electing God" http://pajamasmedia.com/richardfernandez/2009/07/06/electing-god/
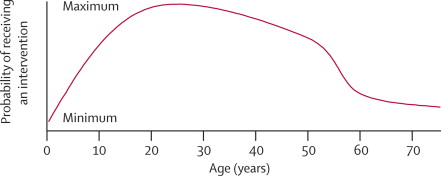
"Because none of the currently used systems satisfy all ethical requirements for just allocation, we propose an alternative: the complete lives system. This system incorporates five principles: youngest-first, prognosis, save the most lives, lottery, and
instrumental value. … When implemented, the complete lives system produces a priority curve on which individuals aged between roughly 15 and 40 years get the most substantial chance, whereas the youngest and oldest people get chances that are attenuated … the complete lives system is least vulnerable to corruption.
Age can be established quickly and accurately from identity documents. Prognosis allocation encourages physicians to improve patients’ health, unlike the perverse incentives to sicken patients or misrepresent health that the sickest-first allocation creates"